

Silent Stroke?
What is the difference with a “silent” stroke?
Strokes are feared because of their neurological results, however the incidence of strokes without appreciable neurological deficits is high. Few people recognise the very strong connection between sleep disordered breathing and stroke!
Abstract: Strokes are feared because of their neurological results, however the incidence of strokes without appreciable neurological deficits is high. Some suggestions are made in regard to prevention and awareness.
AVOIDING SILENT STROKE
Stroke is the sudden reduction or loss of blood flow to a particular region of the brain and when associated with a transient and reversible neurological deficit, (Transient ischemic attack, TIA) or with permanent neurological dysfunction, symptomatic stroke and is termed “silent” when not.
About 20% of strokes are hemorrhagic due to uncontrolled bleeding in the brain, 80% ischemic due to clots.
It is worth noting that patients with obstructive sleep apnea (OSA) represent over 80% of strokes seen. Heavy snoring alone has also shown to be a significant risk factor, (see below) yet neither are generally considered either in prevention or postoperative care.
In Canada six percent of all deaths are due to stroke with 14,000 Canadians dying from stroke annually. There are an estimated 50,000 strokes in Canada each year, that’s one stroke every 10 minutes.
With around 315,000 Canadians living with the effects of stroke, the cost to the Canadian economy is around $3.6 billion per year. Every year, patients with stroke spend more than 639,000 days in acute care in Canadian hospitals and 4.5 million days in residential care facilities

Figures from the UK estimate that approximately 57,000 people experienced a stroke for the first time in 2016. Adjusting to the 2013 European standard population to account for differing age structures resulted in the incidence rate increasing slightly from 1.03 strokes per 1,000 population to 1.13 strokes per 1,000 population. (Public Health England)
Silent strokes (silent brain infarction or SBI ) only affect a small area of the brain, but the damage may be accumulative.
Factors increasing risk and incidence of silent stroke include.
Blood clots
High blood pressure
Narrowed arteries
High cholesterol
Diabetes
Snoring
Obstructive sleep apnea (OSA)
How is is it possible to have a stroke and not know it?
Silent strokes usually display no symptoms at all. Like ischemic strokes, silent strokes happen when blood supply to a part of the brain is suddenly cut off, depriving the brain of oxygen and damaging brain cells.
A silent stroke is, hard to recognize. Because a silent stroke disrupts blood supply to a part of your brain that doesn’t control any visible functions like speaking or moving it is less apparent, so the sufferer might never know a stroke occurred.
Are silent strokes dangerous?
Following several silent strokes, recall and memory may be affected, or difficulty in concentrating. SBI my also increase risk of symptomatic stroke in the future. SBI damage is permanent and effects may be accumulative.
Multiple SBI increases risk for vascular dementia, the symptoms of multi-infarct dementia include:, memory problems, emotional issues, (laughing or crying at inappropriate times), changes to walking gait, getting lost in familiar places, difficulty in decision making, loss of bowel and/or bladder control.
Researchers have known for some time that silent strokes are fairly common, and a serious problem of developed countries. Studies have shown a significant and rapidly increasing prevalence after 65 years of age.
Can you prevent silent strokes ?
Reduction of the chances of a silent of symptomatic stroke is realistic and worthwhile.
Certainly easier to deal with prevention than management of what is in effect irreparable damage.
Stabilize and manage blood pressure. high blood pressure raises your risk for having a silent stroke.
Exercise. One 2011 study showed that 30 minutes of moderate exercise five days a week may reduce your chances of having a silent stroke by up to 40 percent. If you’re physically active, you’ll also have fewer stroke complications and better outcomes than if you’re sedentary. For those that won’t exercise a good walk has its benefits!
Reduce salt intake. The American Stroke Association recommends reduced sodium intake to reduce blood pressure and risk for stroke. Up to 70 percent of your sodium intake is in frozen and prepackaged foods.
Manage your weight. A body mass index of 18.5 to 24.9 is considered normal although it is possible that fat distribution may be the more significant factor.
Lower your cholesterol levels. Current ‘guidelines’ indicate that total cholesterol should be lower than 200 mg/dL. Your HDL (good) cholesterol should ideally be 60 mg/dL or higher. Your LDL (bad) cholesterol should be under 100 mg/dL. Advice changes from time to time and an open mind is suggested.
Quit smoking. If you smoke – quit., for the sake of yourself and those around you. Smoking is associated with an elevated risk for heart disease and stroke in both the smoker and from second hand smoke
Avoid artificially sweetened soft drinks. Drinking artificially sweetened drinks may raise your risk for both dementia and stroke.
Diabetes is a known risk factor of stroke.
Snoring linked to heart attack and and stroke
Increasing evidence suggests that snoring is part of the spectrum of sleep-disordered breathing (SDB), from simple snoring on one end to obstructive sleep apnea/hypopnea syndrome on the other. Snoring is not necessarily benign.
Several studies now confirm that “loud snorers are considerably more likely to develop stroke and heart disease compared to those who never or very rarely snore” and a strong relationship to the development of systemic hypertension.
Clearly if suspected, snoring and/or obstructive sleep apnea should be investigated.
Stroke’s link with depression
Major depression is a risk factor and also a consequence of silent brain infarction (SBI). Persons who present with symptoms of presenile and senile major depression showed a markedly higher incidence of SBI (65.9% and 93.7%).
Individuals with major depression who have had an SBI present with more marked neurological deficits and more severe depressive symptoms than do those without SBI
Stroke and obstructive sleep apnea.
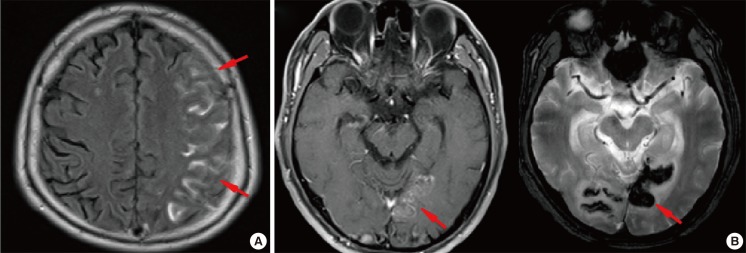
MRI Studies have shown that ‘silent brain infarct’ may occur in up to 25% of patients with moderate to severe OSA.
These patients didn’t know that they’d had a stroke.
In 51 of 56 stroke patients evaluated, OSA was present (91 %) and of these 51 patients, 29 % had severe OSA and 30 %, moderate OSA. 58 % of patients who had suffered an unknown clinically silent infarct were found to have severe OSA.
OSA remains a poorly screened and diagnosed disease of epidemic proportions.
Stroke and antioxidants
Antioxidants are believed to reduce cell damage within the body by countering the potentially dangerous effects of free radicals produced when the body processes oxygen.
CLICK BELOW FOR PROTECTIVE ANTI OXIDANT SUPPLEMENT

Antioxidants are potentially a promising treatment for strokes because they can be given after a stroke occurs to help reduce cell damage.
CLICK BELOW TO RECEIVE YOUR FREE “BETTER SLEEP” GUIDE
