There are other sleep disorders like Restless Legs Syndrome (RLS) which cause fragmentation of sleep. That just means that it ‘messes up’ your normal sleep cycles which you need to be your daytime best . The other reason I mention this, is that OSA can actually cause Insomnia.
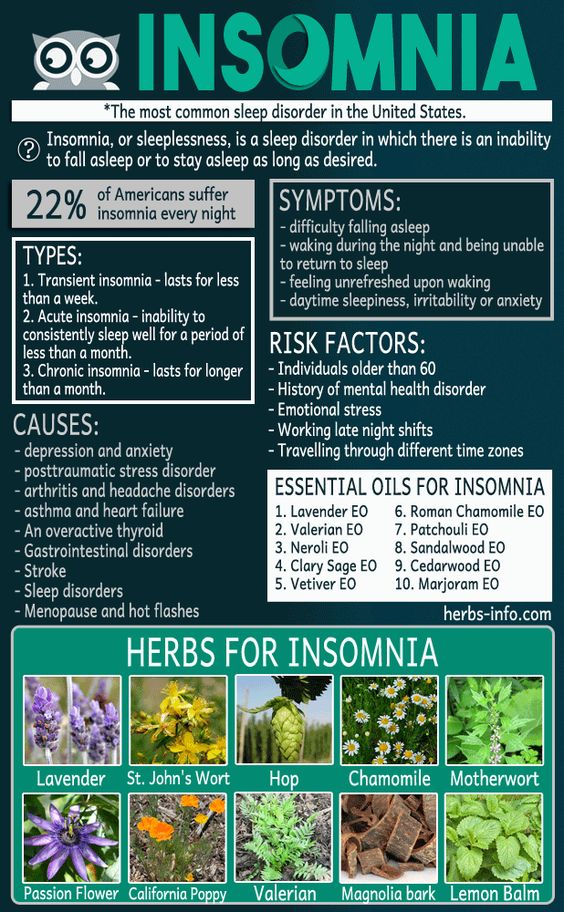
Insomnia
Evidence (and common-sense) shows that choking and the inability to breathe at night often unconsciously (or otherwise), predisposes the sufferer to not want to go to sleep when this potentially fatal disease takes place. After all, if you were strangled every time you went to sleep, you might not be in a hurry to go to sleep either!
Anxiety and depression are frequently seen in association with OSA. Of course, if you’re suffering from insomnia and the resultant signs of sleep deprivation, it’s not likely that you’ll be on top of your game during the day either. Being ‘cranky’ with mood swings is a sign of poor sleep. The good news is that BSM and CBT-I is usually useful even if you have mild to moderate signs of anxiety or depression which makes sense when you think about it. Perhaps not surprisingly, those people may see greater overall benefits too!
But we have to be realistic, there will always be some for whom this won’t work – who are they?
So, those with Insomnia may also have SDB. Obviously if this is a component, failure to treat the SDB will likely compromise your Sleep Quality and likely resolution of Insomnia too.
Of course, it also leaves the SDB sufferer (or their bedpartner) vulnerable to the consequences of that disorder.
OSA is heavily associated with High Blood Pressure (Hypertension), Heart Attack,
Stroke and Diabetes. As mentioned earlier Anxiety, Depression and Mood-Disorders are often associated.
Decision making and cognitive function are (not surprisingly) affected and the chance of a car crash is increased in those that have just moderate Obstructive Sleep Apnea, by op to 7 times the rate of healthy sleepers.
While there are different management tools for SDB, you will need to find someone who is not selling you their particular management tool, be it CPAP (mask, hose and pump), Oral or dental device (OAT), laser, surgery or one of a million unproven devices out there that border on snake oil sold by charlatans without any regulation, or on their part, often ethics either. However, having said that, management is crucial and for some it will be like having a new life, just be sure to ask questions. Unfortunately, even physicians can be heavily biased.

I also mentioned it was generally OK to use CBT-I to treat insomnia in those with mild to moderate anxiety and/or depression . If someone has serious (major) depression so that they are unable to work, find no pleasure in life and may even have suicidal thoughts, jumping over such issues to address insomnia management first may be dangerous. Cases of severe anxiety, depression or other mood problems should be reviewed by your physician. Bi-polar disorder is another example that affects sleep. Studies show poor medical recognition of Bi-polar Disorder, just as there is poor medical awareness of SDB.
Your family physician should always be your first port of call for these disorders in order that you can get care by referral, which may include counselling, psychotherapy, CBT or even medicines (usually not sleeping tablets). It is important not to overlook the presence of these issues, especially in someone suffering from insomnia.
What are some of the other issues that we should be aware of?